
Stellate ganglion block reduces symptoms of Long COVID: A case series
Short communication – Journal of neuroimmunology
Luke D. Liu, Deborah L. Duricka * Neuroversion Inc., Anchorage, AK, USA ARTICLE INFO
Keywords: Long COVID/PASC Myalgic encephalitis/chronic fatigue syndrome (ME/CFS) Postural orthopedic tachycardia syndrome (POTS) Dysautonomia Stellate ganglion block Cerebral blood flow
ABSTRACT After recovering from COVID-19, a significant proportion of symptomatic and asymptomatic individuals develop Long COVID. Fatigue, orthostatic intolerance, brain fog, anosmia, and ageusia/dysgeusia in Long COVID resemble “sickness behavior,” the autonomic nervous system response to pro-inflammatory cytokines (Dantzer et al., 2008). Aberrant network adaptation to sympathetic/parasympathetic imbalance is expected to produce long-standing dysautonomia. Cervical sympathetic chain activity can be blocked with local anesthetic, allowing the regional autonomic nervous system to “reboot.” In this case series, we successfully treated two Long COVID patients using stellate ganglion block, implicating dysautonomia in the pathophysiology of Long COVID and suggesting a novel treatment.
__________________________________________________________________________________
Post COVID-19 syndrome associated with orthostatic cerebral hypoperfusion syndrome, small fiber neuropathy and benefit of immunotherapy: a case report
Peter Novak 1
eNeurologicalSci . 2020 Dec;21:100276.
doi: 10.1016/j.ensci.2020.100276. Epub 2020 Sep 20.
PMID: 32984564PMCID: PMC7502253
Abstract
Coronavirus disease (COVID-19) is a novel highly contagious infectious disease caused by the coronavirus SARS-CoV2. The virus affects the human respiratory and other systems, and presents mostly as acute respiratory syndrome with fever, fatigue, dry cough, myalgia and dyspnea. The clinical manifestations vary from no symptoms to multiple organ failure. Majority of patients fully recover. Several postinfectious presumably autoimmune complications of COVID-19 affecting the brain or peripheral large nerve fibers have been reported. This report describes a post COVID-19 patient who developed chronic fatigue, orthostatic dizziness and brain fog consistent with orthostatic hypoperfusion syndrome (OCHOS), a form of orthostatic intolerance, and painful small fiber neuropathy (SFN). Initially, the patient was diagnosed with. OCHOS (detected by the tilt test with transcranial Doppler monitoring) and SFN (confirmed by skin biopsy), and both OCHOS/SFN were attributed to Post Treatment Lyme Disease Syndrome of presumed autoimmune etiology. Patient recovered on symptomatic therapy. COVID-19 triggered exacerbation of OCHOS/SFN responded to immunotherapy with intravenous immunoglobulins. This case suggests that post COVID-19 syndrome may present as an autoimmune OCHOS/SFN and that early immunotherapy may be effective. Further studies are necessary to confirm the link between OCHOS/SFN and COVID-19 disease as well as to confirm the benefit of immunotherapy.
© 2020 Published by Elsevier B.V.
__________________________________________________________________________________
PLoS One
2019 Feb 12;14(2):e0212222. doi: 10.1371/journal.pone.0212222. eCollection 2019.
Association of small fiber neuropathy and post treatment Lyme disease syndrome
Peter Novak 1, Donna Felsenstein 2, Charlotte Mao 3, Nadlyne R Octavien 4, Nevena Zubcevik 5
PMID: 30753241 PMCID: PMC6372188
Abstract
Objectives: To examine whether post-treatment Lyme disease syndrome (PTLDS) defined by fatigue, cognitive complaints and widespread pain following the treatment of Lyme disease is associated with small fiber neuropathy (SFN) manifesting as autonomic and sensory dysfunction.
Methods: This single center, retrospective study evaluated subjects with PTLDS. Skin biopsies for assessment of epidermal nerve fiber density (ENFD), sweat gland nerve fiber density (SGNFD) and functional autonomic testing (deep breathing, Valsalva maneuver and tilt test) were performed to assess SFN, severity of dysautonomia and cerebral blood flow abnormalities. Heart rate, end tidal CO2, blood pressure, and cerebral blood flow velocity (CBFv) from middle cerebral artery using transcranial Doppler were monitored.
Results: 10 participants, 5/5 women/men, age 51.3 ± 14.7 years, BMI 27.6 ± 7.3 were analyzed. All participants were positive for Lyme infection by CDC criteria. At least one skin biopsy was abnormal in all ten participants. Abnormal ENFD was found in 9 participants, abnormal SGNFD in 5 participants, and both abnormal ENFD and SGNFD were detected in 4 participants. Parasympathetic failure was found in 7 participants and mild or moderate sympathetic adrenergic failure in all participants. Abnormal total CBFv score was found in all ten participants. Low orthostatic CBFv was found in 7 participants, three additional participants had abnormally reduced supine CBFv.
Conclusions: SFN appears to be associated with PTLDS and may be responsible for certain sensory symptoms. In addition, dysautonomia related to SFN and abnormal CBFv also seem to be linked to PTLDS. Reduced orthostatic CBFv can be associated with cerebral hypoperfusion and may lead to cognitive dysfunction. Autonomic failure detected in PTLDS is mild to moderate. SFN evaluation may be useful in PTLDS.
__________________________________________________________________________________
Diverse functional autoantibodies in patients with COVID-19
Eric Y Wang # 1, Tianyang Mao # 1, Jon Klein # 1, Yile Dai # 1, John D Huck 1, Jillian R Jaycox 1, Feimei Liu 1, Ting Zhou 1, Benjamin Israelow 1, Patrick Wong 1, Andreas Coppi 2, Carolina Lucas 1, Julio Silva 1, Ji Eun Oh 1, Eric Song 1, Emily S Perotti 1, Neil S Zheng 1, Suzanne Fischer 1, Melissa Campbell 3, John B Fournier 3, Anne L Wyllie 4, Chantal B F Vogels 4, Isabel M Ott 4, Chaney C Kalinich 4, Mary E Petrone 4, Anne E Watkins 4, Yale IMPACT Team; Charles Dela Cruz 5, Shelli F Farhadian 3, Wade L Schulz 2 6, Shuangge Ma 7, Nathan D Grubaugh 4, Albert I Ko 3 4, Akiko Iwasaki 8 9 10, Aaron M Ring 11 12
PMID: 34010947 DOI: 10.1038/s41586-021-03631-y
Nature 2021 Jul;595(7866):283-288. doi: 10.1038/s41586-021-03631-y. Epub 2021 May 19
Abstract
COVID-19 manifests with a wide spectrum of clinical phenotypes that are characterized by exaggerated and misdirected host immune responses1-6. Although pathological innate immune activation is well-documented in severe disease1, the effect of autoantibodies on disease progression is less well-defined. Here we use a high-throughput autoantibody discovery technique known as rapid extracellular antigen profiling7 to screen a cohort of 194 individuals infected with SARS-CoV-2, comprising 172 patients with COVID-19 and 22 healthcare workers with mild disease or asymptomatic infection, for autoantibodies against 2,770 extracellular and secreted proteins (members of the exoproteome). We found that patients with COVID-19 exhibit marked increases in autoantibody reactivities as compared to uninfected individuals, and show a high prevalence of autoantibodies against immunomodulatory proteins (including cytokines, chemokines, complement components and cell-surface proteins). We established that these autoantibodies perturb immune function and impair virological control by inhibiting immunoreceptor signalling and by altering peripheral immune cell composition, and found that mouse surrogates of these autoantibodies increase disease severity in a mouse model of SARS-CoV-2 infection. Our analysis of autoantibodies against tissue-associated antigens revealed associations with specific clinical characteristics. Our findings suggest a pathological role for exoproteome-directed autoantibodies in COVID-19, with diverse effects on immune functionality and associations with clinical outcomes.
__________________________________________________________________________________
ORIGINAL RESEARCH article
Front. Syst. Neurosci., 01 September 2021 | https://doi.org/10.3389/fnsys.2021.698240
Acute Corticotropin-Releasing Factor Receptor Type 2 Agonism Results in Sustained Symptom Improvement in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
Gerard Pereira1*, Hunter Gillies1, Sanjay Chanda1, Michael Corbett1, Suzanne D. Vernon2, Tina Milani2 and Lucinda Bateman2
Cortene Inc., Burlingame, CA, United States 2Bateman Horne Center, Salt Lake City, UT,
Background: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a complex multi-symptom disease with widespread evidence of disrupted systems. The authors hypothesize that it is caused by the upregulation of the corticotropin-releasing factor receptor type 2 (CRFR2) in the raphé nuclei and limbic system, which impairs the ability to maintain homeostasis. The authors propose utilizing agonist-mediated receptor endocytosis to downregulate CRFR2.
Materials and Methods: This open-label trial tested the safety, tolerability and efficacy of an acute dose of CT38s (a short-lived, CRFR2-selective agonist, with no known off-target activity) in 14 ME/CFS patients. CT38s was subcutaneously-infused at one of four dose-levels (i.e., infusion rates of 0.01, 0.03, 0.06, and 0.20 μg/kg/h), for a maximum of 10.5 h. Effect was measured as the pre-/post-treatment change in the mean 28-day total daily symptom score (TDSS), which aggregated 13 individual patient-reported symptoms.
Results: ME/CFS patients were significantly more sensitive to the transient hemodynamic effects of CRFR2 stimulation than healthy subjects in a prior trial, supporting the hypothesized CRFR2 upregulation. Adverse events were generally mild, resolved without intervention, and difficult to distinguish from ME/CFS symptoms, supporting a CRFR2 role in the disease. The acute dose of CT38s was associated with an improvement in mean TDSS that was sustained (over at least 28 days post-treatment) and correlated with both total exposure and pre-treatment symptom severity. At an infusion rate of 0.03 μg/kg/h, mean TDSS improved by −7.5 ± 1.9 (or −25.7%, p = 0.009), with all monitored symptoms improving.
Conclusion: The trial supports the hypothesis that CRFR2 is upregulated in ME/CFS, and that acute CRFR2 agonism may be a viable treatment approach warranting further study.
International Journal of Environmental Research and Public Health
__________________________________________________________________________________
Impact of Life Stressors on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Symptoms: An Australian Longitudinal Study
Cassandra Balinas 1,2,3,†, Natalie Eaton-Fitch 1,2,3,†, Rebekah Maksoud 1,2,* ,† , Donald Staines 1,2 and Sonya Marshall-Gradisnik 1,2 Citation: Balinas, C.; Eaton-Fitch, N.; Maksoud, R.; Staines, D.; Marshall-Gradisnik, S. Impact of Life Stressors on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Symptoms: An Australian Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 10614. https://doi.org/10.3390/ ijerph182010614 Academic Editor: Paul B. Tchounwou Received: 1 September 2021 Accepted: 6 October 2021 Published: 11 October 2021
The National Centre for Neuroimmunology and Emerging Diseases, Menzies Health Institute Queensland, Griffith University, Gold Coast 4215, Australia;
Abstract: (1) Background: Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a complex, multifaceted illness. The pathomechanism, severity and progression of this illness is still being investigated. Stressors have been implicated in symptom exacerbation for ME/CFS, however, there is limited information for an Australian ME/CFS cohort. The aim of this study was to assess the potential effect of life stressors including changes in work, income, or family scenario on symptom severity in an Australian ME/CFS cohort over five months; (2) Methods: Australian residents with ME/CFS responded to questions relating to work, income, living arrangement, access to healthcare and support services as well as symptoms experienced; (3) Results: thirty-six ME/CFS patients (age: 41.25 ± 12.14) completed all questionnaires (response rate 83.7%). Muscle pain and weakness, orthostatic intolerance and intolerance to extreme temperatures were experienced and fluctuated over time. Sleep disturbances were likely to present as severe. Work and household income were associated with worsened cognitive, gastrointestinal, body pain and sleep symptoms. Increased access to healthcare services was associated with improved symptom presentation; (4) Conclusions: life stressors such as work and financial disruptions may significantly contribute to exacerbation of ME/CFS symptoms. Access to support services correlates with lower symptom scores.
__________________________________________________________________________________
The impact of COVID-19 critical illness on new disability, functional outcomes and return to work at 6 months: a prospective cohort study
Carol L. Hodgson, Alisa M. Higgins,
The COVID-Recovery Study Investigators and the ANZICS Clinical Trials Group
Critical Care volume 25, Article number: 382 (2021) Published: 08 November 2021
Abstract
Background
There are few reports of new functional impairment following critical illness from COVID-19. We aimed to describe the incidence of death or new disability, functional impairment and changes in health-related quality of life of patients after COVID-19 critical illness at 6 months.
Methods
In a nationally representative, multicenter, prospective cohort study of COVID-19 critical illness, we determined the prevalence of death or new disability at 6 months, the primary outcome. We measured mortality, new disability and return to work with changes in the World Health Organization Disability Assessment Schedule 2.0 12L (WHODAS) and health status with the EQ5D-5LTM.
Results
Of 274 eligible patients, 212 were enrolled from 30 hospitals. The median age was 61 (51–70) years, and 124 (58.5%) patients were male. At 6 months, 43/160 (26.9%) patients died and 42/108 (38.9%) responding survivors reported new disability. Compared to pre-illness, the WHODAS percentage score worsened (mean difference (MD), 10.40% [95% CI 7.06–13.77]; p < 0.001). Thirteen (11.4%) survivors had not returned to work due to poor health. There was a decrease in the EQ-5D-5LTM utility score (MD, − 0.19 [− 0.28 to − 0.10]; p < 0.001). At 6 months, 82 of 115 (71.3%) patients reported persistent symptoms. The independent predictors of death or new disability were higher severity of illness and increased frailty.
Conclusions
At six months after COVID-19 critical illness, death and new disability was substantial. Over a third of survivors had new disability, which was widespread across all areas of functioning.
Clinical trial registration NCT04401254 May 26, 2020.
__________________________________________________________________________________
Submaximal Exercise Provokes Increased Activation of the Anterior Default Mode Network During the Resting State as a Biomarker of Postexertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
Rakib U. Rayhan and James N. Baraniuk
Abstract
Background: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is characterized by disabling fatigue and postexertiona*l malaise. We developed a provocation paradigm with two submaximal bicycle exercise stress tests on consecutive days bracketed by magnetic resonance imaging, orthostatic intolerance, and symptom assessments before and after exercise in order to induce objective changes of exercise induced symptom exacerbation and cognitive dysfunction.
Method: Blood oxygenation level dependent (BOLD) scans were performed while at rest on the preexercise and postexercise days in 34 ME/CFS and 24 control subjects. Seed regions from the FSL data library with significant BOLD signals were nodes that clustered into networks using independent component analysis. Differences in signal amplitudes between groups on pre- and post-exercise days were determined by general linear model and ANOVA.
Results: The most striking exercise-induced effect in ME/CFS was the increased spontaneous activity in the medial prefrontal cortex that is the anterior node of the Default Mode Network (DMN). In contrast, this region had decreased activation for controls. Overall, controls had higher BOLD signals suggesting reduced global cerebral blood flow in ME/CFS.
Conclusion: The dynamic increase in activation of the anterior DMN node after exercise may be a biomarker of postexertional malaise and symptom exacerbation in CFS. The specificity of this postexertional finding in ME/CFS can now be assessed by comparison to post-COVID fatigue, Gulf War Illness, fibromyalgia, chronic idiopathic fatigue, and fatigue in systemic medical and psychiatric diseases.
Keywords: postexertional malaise, default mode network, DMN, blood oxygenation level dependent, BOLD, fibromyalgia, chronic idiopathic fatigue, submaximal exercise
__________________________________________________________________________________
Insights into Metabolite Diagnostic Biomarkers for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
Emi Yamano, Yasuyoshi Watanabe, and Yosky Kataoka
Abstract
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a persistent and unexplained pathological state characterized by exertional and severely debilitating fatigue, with/without infectious or neuropsychiatric symptoms, and with a minimum duration of 6 consecutive months. Its pathogenesis is not fully understood. There are no firmly established diagnostic biomarkers or treatment, due to incomplete understanding of the etiology of ME/CFS and diagnostic uncertainty. Establishing a biomarker for the objective diagnosis is urgently needed to treat a lot of patients. Recently, research on ME/CFS using metabolome analysis methods has been increasing. Here, we overview recent findings concerning the metabolic features in patients with ME/CFS and the animal models which contribute to the development of diagnostic biomarkers for ME/CFS and its treatment. In addition, we discuss future perspectives of studies on ME/CFS.
Keywords: ME/CFS, etiology, biomarker, metabolome, objective diagnosis
__________________________________________________________________________________
TRYPTOPHAN METABOLITES, CYTOKINES, AND FATTY ACID BINDING PROTEIN 2 IN MYALGIC ENCEPHALOMYELITIS/CHRONIC FATIGUE SYNDROME –
PROF. ALDO BARITUSSIO ET AL
Abstract
Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) differ for triggers, mode of start, associated symptoms, evolution, and biochemical traits. Therefore, serious attempts are underway to partition them into subgroups useful for a personalized medicine approach to the disease.
Here, we investigated clinical and biochemical traits in 40 ME/CFS patients and 40 sex- and age-matched healthy controls.
Particularly, we analyzed serum levels of some cytokines, Fatty Acid Binding Protein 2 (FAPB-2), tryptophan, and some of its metabolites via serotonin and kynurenine.
ME/CFS patients were heterogeneous for genetic background, trigger, start mode, symptoms, and evolution. ME/CFS patients had higher levels of IL-17A (p = 0.018), FABP-2 (p = 0.002), and 3-hydroxykynurenine (p = 0.037) and lower levels of kynurenine (p = 0.012) and serotonin (p = 0.045) than controls.
Changes in kynurenine and 3-hydroxykynurenine were associated with increased kynurenic acid/kynurenine and 3-hydroxykynurenine/kynurenine ratios, indirect measures of kynurenine aminotransferases and kynurenine 3-monooxygenase enzymatic activities, respectively.
No correlation was found among cytokines, FABP-2, and tryptophan metabolites, suggesting that inflammation, anomalies of the intestinal barrier, and changes of tryptophan metabolism may be independently associated with the pathogenesis of the disease.
Interestingly, patients with the start of the disease after infection showed lower levels of kynurenine (p = 0.034) than those not starting after an infection. Changes in tryptophan metabolites and increased IL-17A levels in ME/CFS could both be compatible with anomalies in the sphere of energy metabolism.
Overall, clinical traits together with serum biomarkers related to inflammation, intestine function, and tryptophan metabolism deserve to be further considered for the development of personalized medicine strategies for ME/CFS.
__________________________________________________________________________________
BACK TO THE FUTURE? IMMUNOGLOBULIN THERAPY FOR MYALGIC ENCEPHALOMYELITIS/CHRONIC FATIGUE SYNDROME
Helen Brownlie and Nigel Speight
ABSTRACT
The findings of controlled trials on use of intravenous immunoglobulin G (IV IgG) to treat myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are generally viewed as representing mixed results. On detailed review, a clearer picture emerges, which suggests that the potential therapeutic value of this intervention has been underestimated.
Our analysis is consistent with the propositions that:
(1) IgG is highly effective for a proportion of patients with severe and well-characterised ME/CFS;
(2) responders can be predicted with a high degree of accuracy based on markers of immune dysfunction.
Rigorous steps were taken in the research trials to record adverse events, with transient symptom exacerbation commonly experienced in both intervention and placebo control groups, suggesting that this reflected the impact of participation on people with an illness characterised by post-exertional symptom exacerbation.
Worsening of certain specific symptoms, notably headache, did occur more commonly with IgG and may have been concomitant to effective treatment, being associated with clinical improvement.
The findings emerging from this review are supported by clinical observations relating to treatment of patients with severe and very severe ME/CFS, for whom intramuscular and subcutaneous administration provide alternative options.
We conclude that: (1) there is a strong case for this area of research to be revived;
(2) pending further research, clinicians would be justified in offering a course of IgG to selected ME/CFS patients at the more severe end of the spectrum. As the majority of trial participants had experienced an acute viral or viral-like onset, we further suggest that IgG treatment may be pertinent to the care of some patients who remain ill following infection with SARS-CoV-2 virus
Free full text: Healthcare
__________________________________________________________________________________
A Possible Role for Anti-idiotype Antibodies in SARS-CoV-2 Infection and Vaccination published on November 24, 2021, at NEJM.org.
William J. Murphy, Ph.D., and Dan L. Longo, M.D.
The pathogenesis of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is incompletely understood, with its effects on multiple organ systems1 and the syndrome of “long Covid” occurring long after the resolution of infection.2 The development of multiple efficacious vaccines has been critical in the control of the pandemic, but their efficacy has been limited by the appearance of viral variants, and the vaccines can be associated with rare off-target or toxic effects, including allergic reactions, myocarditis, and immune-mediated thrombosis and thrombocytopenia in some healthy adults. Many of these phenomena are likely to be immune-mediated.3 How can we understand this diversity in immune responses in different persons?
One way of thinking about the complexity of the immune response is through the lens of anti-idiotype immune responses. The Network Hypothesis, formulated in 1974 by Niels Jerne, described a mechanism by which the antibody responses to an antigen themselves induced downstream antibody responses against the antigen-specific antibody.4 Every antibody that is induced and specific for an antigen (termed “Ab1” antibody) has immunogenic regions, particularly in their variable-region antigen-binding domains, that are unique as a result of genetic recombination of immunoglobulin variable, diversity, and joining (VDJ) genes; VDJ recombination results in new and therefore immunogenic amino acid sequences called idiotopes, which are then capable of inducing specific antibodies against Ab1 antibodies as a form of down-regulation. A similar paradigm has been proposed for T cells. However, these regulatory immune responses are also capable of doing much more. The paratopes, or antigen-binding domains, of some of the resulting anti-idiotype (or “Ab2”) antibodies that are specific for Ab1 can structurally resemble that of the original antigens themselves. Thus, the Ab2 antigen-binding region can potentially represent an exact mirror image of the initial targeted antigen in the Ab1 response, and Ab2 antibodies have even been examined for potential use as a surrogate for the antigen in vaccine studies. However, as a result of this mimicry, Ab2 antibodies also have the potential to bind the same receptor that the original antigen was targeting (Figure 1). Ab2 antibodies binding to the original receptor on normal cells therefore have the potential to mediate profound effects on the cell that could result in pathologic changes, particularly in the long term — long after the original antigen itself has disappeared.
This aspect of regulation of immune-cell responses was postulated by Plotz in 1983 as a possible cause of autoimmunity arising after viral infection5 and has since been supported experimentally by direct transfer of anti-idiotype antibodies. Ab2 antibodies generated against the enterovirus coxsackievirus B3 in mice can bind myocyte antigens, resulting in autoimmune myocarditis,6 and anti-idiotype responses can act as acetylcholine receptor agonists, leading to myasthenia gravis symptoms in rabbits.7 In addition, by displaying the mirror image of the viral antigen, Ab2 alone can even mimic the deleterious effects of the virus particle itself, as has been shown with bovine viral diarrhea virus antigen.8
For SARS-CoV-2 infection, attention centers on the spike (S) protein and its critical use of the angiotensin-converting–enzyme 2 (ACE2) receptor to gain entry into the cell. Given its critical role in regulating angiotensin responses, many physiological effects can be influenced by ACE2 engagement.9 The S protein itself has a direct effect on suppressing ACE2 signaling by a variety of mechanisms and can also directly trigger toll-like receptors and induce inflammatory cytokines.10 Anti-idiotype responses may affect ACE2 function, resulting in similar effects. However, preclinical and clinical assessments of antibody responses to SARS-CoV-2 vaccines have focused solely on Ab1 responses and virus-neutralizing efficacy. The delineation of potential anti-idiotype responses has inherent difficulties because of the polyclonal nature of responses, dynamic kinetics, and the concurrent presence of both Ab1 and Ab2 antibodies. Furthermore, ACE2 expression within cells and tissues can be variable. The different vaccine constructs (RNA, DNA, adenoviral, and protein) are also likely to have differential effects on Ab2 induction or in the mediation of vaccine effects that differ from responses to infection. Some off-target effects may not be directly linked to Ab2 responses. The association of thrombotic events with some SARS-CoV-2 vaccines in young women and the etiologic role of anti–platelet factor 4–polyanion antibodies may be the result of the adenoviral vector. However, the reported occurrence of myocarditis after vaccine administration bears striking similarities to the myocarditis associated with Ab2 antibodies induced after some viral infections.6 Ab2 antibodies could also mediate neurologic effects of SARS-CoV-2 infection or vaccines, given the expression of ACE2 on neuronal tissues, the specific neuropathologic effects of SARS-CoV-2 infection,11 and the similarity of these effects to Ab2-mediated neurologic effects observed in other viral models.
It would therefore be prudent to fully characterize all antibody and T-cell responses to the virus and the vaccines, including Ab2 responses over time. Using huACE2 transgenic mice and crossing them with strains that are predisposed to autoimmunity or other human pathologic conditions can also provide important insights. An understanding of potential Ab2 responses may also provide insights into Ab1 maintenance and efficacy and into the application of antibody-based therapeutic agents. However, much more basic science research is needed to determine the potential role idiotype-based immunoregulation of both humoral and cell-mediated responses may play both in antiviral efficacy and in unwanted side effects of both SARS-CoV-2 infection and the vaccines that protect us from it.
__________________________________________________________________________________
Graded exercise therapy for ME/CFS: finding consensus between the royal colleges, patients, and researchers
BMJ 2021; 375 doi: https://doi.org/10.1136/bmj.n3026 (Published 08 December 2021)Cite this as: BMJ 2021;375:n3026
The BMJ reports the royal colleges’ discontent with the new National Institute for Health and Care Excellence guideline on myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome (ME/CFS), particularly regarding graded exercise therapy (GET).12 The quality of the evidence and the rigour of its assessment are contested by the colleges, patient representatives, and researchers.34 In summary, the colleges emphasise the potential benefits of exercise for patients with ME/CFS, the patient community emphasises the potential harm that exercise can cause, and both communities quote research supporting their hypotheses, the quality of which is contested. Is there any agreement on the guideline?
Consider a patient with ME/CFS who, after attempting a therapy based on exercise, reports a worsening of their symptoms, sequelae which they regard as harmful. Should the treating physician interpret this as “the bodies [sic] normal response” and press on? Or should they defer to the NICE assertion that “treatment programmes that result in symptom exacerbation are not recommended” and abandon exercise based approaches?5
The guideline is quite clear: “Health and social care professionals should take time to build supportive, trusting, and empathetic relationships.” Trust cannot be achieved if a patient believes the prescribed treatment is causing them harm. Surely royal colleges, researchers, and patients can all agree on this?
__________________________________________________________________________________
SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19
Lize M. Grobbelaar, Sample analysis, Visualization, Writing—original draft, Chantelle Venter, Data curation, Project administration, [...], and Etheresia Pretorius,
Bioscience reports Volume 41, Issue 8 – August 2021
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2)-induced infection, the cause of coronavirus disease 2019 (COVID-19), is characterized by unprecedented clinical pathologies. One of the most important pathologies, is hypercoagulation and microclots in the lungs of patients. Here we study the effect of isolated SARS-CoV-2 spike protein S1 subunit as potential inflammagen sui generis. Using scanning electron and fluorescence microscopy as well as mass spectrometry, we investigate the potential of this inflammagen to interact with platelets and fibrin(ogen) directly to cause blood hypercoagulation.
Using platelet-poor plasma (PPP), we show that spike protein may interfere with blood flow. Mass spectrometry also showed that when spike protein S1 is added to healthy PPP, it results in structural changes to β and γ fibrin(ogen), complement 3, and prothrombin. These proteins were substantially resistant to trypsinization, in the presence of spike protein S1. Here we suggest that, in part, the presence of spike protein in circulation may contribute to the hypercoagulation in COVID-19 positive patients and may cause substantial impairment of fibrinolysis. Such lytic impairment may result in the persistent large microclots we have noted here and previously in plasma samples of COVID-19 patients. This observation may have important clinical relevance in the treatment of hypercoagulability in COVID-19 patients.
Keywords: COVID-19, electron microscopy, Fibrin(ogen), fluorescence microscopy, Microclot, Spike protein Sa
__________________________________________________________________________________
MEDICAL NEWS: New metabolic phenotype of long COVID identified
Heather Mason | 18 January 2022
A potential new cluster phenotype for patients with post-acute COVID syndrome (PACS) is described in an article published in Open Forum Infectious Diseases, which reports on the prevalence of this metabolic-associated fatty liver disease (MAFLD) phenotype.
The analysis included 235 patients who were followed at a single university outpatient clinic. The primary outcome was the prevalence of MAFLD, detected by transient elastography, during the first post-discharge follow-up visit, compared with the MAFLD prevalence at the time of hospital admission. Figures were calculated retrospectively using the hepatic steatosis index.
The results showed that the prevalence of MAFLD was 55.3 per cent at follow-up and 37.3 per cent on admission. Among the independent predictors of MAFLD were insulin resistance (odds ratio [OR] 1.5), body mass index (OR 1.14), and metabolic syndrome (OR 2.54).
Regarding a possible link with other clusters, the researchers found that MAFLD had weak or very weak associations, indicating that it may represent an independent PACS cluster, with potential metabolic and cardiovascular health consequences in the long-COVID-19.
The authors highlight the importance of careful follow-up of patients with MAFLD in the context of PACS since it is necessary to understand the clinical implications of this syndrome.
__________________________________________________________________________________
Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis
KJETIL BJORNEVIK HTTPS://ORCID.ORG/0000-0002-2892-6986MARIANNA CORTESE HTTPS://ORCID.ORG/0000-0002-3665-2006BRIAN C. HEALY HTTPS://ORCID.ORG/0000-0001-5272-2425JENS KUHLEMICHAEL J. MINA HTTPS://ORCID.ORG/0000-0002-0674-5762YUMEI LENG HTTPS://ORCID.ORG/0000-0003-2512-9284STEPHEN J. ELLEDGE HTTPS://ORCID.ORG/0000-0001-7923-6283DAVID W. NIEBUHRANN I. SCHER[...]ALBERTO ASCHERIO
SCIENCE • 13 Jan 2022 • Vol 375, Issue 6578 • pp. 296-301 • DOI: 10.1126/science.abj8222
Stronger evidence for viral connection
Multiple sclerosis is a chronic demyelinating disease of the central nervous system. The underlying cause of this disease is not known, but Epstein-Barr virus is thought to be a possible culprit. However, most people infected with this common virus do not develop multiple sclerosis, and it is not feasible to directly demonstrate causation of this disease in humans. Using data from millions of US military recruits monitored over a 20-year period, Bjornevik et al. determined that Epstein-Barr virus infection greatly increased the risk of subsequent multiple sclerosis and that it preceded the development of disease, supporting its potential role in the pathogenesis of multiple sclerosis (see the Perspective by Robinson and Steinman). —YN
Abstract
Multiple sclerosis (MS) is a chronic inflammatory demyelinating disease of the central nervous system of unknown etiology. We tested the hypothesis that MS is caused by Epstein-Barr virus (EBV) in a cohort comprising more than 10 million young adults on active duty in the US military, 955 of whom were diagnosed with MS during their period of service. Risk of MS increased 32-fold after infection with EBV but was not increased after infection with other viruses, including the similarly transmitted cytomegalovirus. Serum levels of neurofilament light chain, a biomarker of neuroaxonal degeneration, increased only after EBV seroconversion. These findings cannot be explained by any known risk factor for MS and suggest EBV as the leading cause of MS.
__________________________________________________________________________________
FDA OKs New Adult Insomnia Med - Medscape medical news
Erik Greb
January 10, 2022
The US Food and Drug Administration (FDA) has approved the dual orexin receptor antagonist daridorexant (Quviviq) for the treatment of insomnia in adults, the drug's manufacturer, Idorsia, has announced.
The FDA's decision was based partly on a phase 3 trial of adults with moderate-to-severe insomnia who were randomly assigned to receive 25 or 50 mg of daridorexant or matching placebo. Daridorexant was associated with dose-dependent improvements in wake after sleep onset, total sleep time, and latency to persistent sleep.
Whereas the overall results are very positive, the improvements in daytime functioning are especially "exciting," Thomas Roth, PhD, director of the Sleep Disorders and Research Center at Henry Ford Hospital in Detroit, Michigan, told Medscape Medical News.
"That's sort of a big deal. For me, that's the biggest deal there is," said Roth, who was a consultant on the design of the phase 3 trial and on the interpretation of the data.
The drug will be available in doses of 25 mg and 50 mg, and the FDA has recommended that it be classified as a controlled substance. After it is scheduled by the US Drug Enforcement Administration, daridorexant is expected to be made available in May.
Favorable Safety Profile
Insomnia is a common disorder characterized by difficulty falling asleep or staying asleep and by early morning awakenings. Patients with insomnia often report fatigue, irritability, and difficulty with concentration. The condition can also result in significant problems with work and social activities, thus contributing to anxiety or depression.
As with other dual orexin receptor antagonists, daridorexant competitively binds with both orexin receptors in the lateral hypothalamus to block the activity of orexin in a reversible way. This approach decreases the downstream action of the wake-promoting neurotransmitters that are overactive in patients with insomnia.
The phase 3 trial measured daytime functioning using the new Insomnia Daytime Symptoms and Impacts Questionnaire (IDSIQ), a patient-reported outcome instrument. Daridorexant was associated with significant improvements in daytime function, particularly in sleepiness and mood.
Previous trials of other dual orexin receptor antagonists did not use the IDSIQ as an outcome, so it is not possible to compare daridorexant with those drugs in this respect, Roth noted. Researchers also have not conducted head-to-head trials of the drug with other dual orexin receptor antagonists.
Daridorexant also had a favorable safety profile and was not associated with rebound insomnia or withdrawal effects. The most common adverse events were headache and somnolence or fatigue.
"They had no effect on sleep stage distribution [and] they had no significant effects on sleep and breathing in people with mild to moderate sleep apnea," said Roth, who presented the phase 3 findings at SLEEP 2020.
__________________________________________________________________________________
The Lancet: ARTICLES| VOLUME 21, ISSUE 2, P125-139, FEBRUARY 01, 2022
Safety and efficacy of daridorexant in patients with insomnia disorder: results from two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials
Summary
Background
Daytime functioning is impaired in people with insomnia disorder. Currently available dual orexin receptor antagonists have shown efficacy in insomnia disorder, but do not address all aspects of this disease. We aimed to assess safety and efficacy of daridorexant, a novel orexin receptor antagonist, on night-time and daytime symptoms of insomnia.
Methods
We did two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials at 156 sites in 17 countries. Adults (aged ≥18 years) with insomnia disorder were randomly assigned using interactive response technology (1:1:1) to receive daridorexant 50 mg, 25 mg, or placebo (study 1) or daridorexant 25 mg, 10 mg, or placebo (study 2) every evening for 3 months. Participants, investigators, and site personnel were masked to treatment allocation. The primary endpoints were change from baseline in wake time after sleep onset (WASO) and latency to persistent sleep (LPS), measured by polysomnography, at months 1 and 3. The secondary endpoints were change from baseline in self-reported total sleep time and the sleepiness domain score of the Insomnia Daytime Symptoms and Impacts Questionnaire (IDSIQ) at months 1 and 3. Study-wise type I error rate (5%) was controlled for all pairwise comparisons. Efficacy was analysed in all randomly assigned participants, and safety in all participants who received at least one dose of treatment. The studies are registered at ClinicalTrials.gov, NCT03545191 (study 1) and NCT03575104 (study 2).
Findings
Between June 4, 2018 and Feb 25, 2020, 930 participants were randomly assigned to receive daridorexant 50 mg (n=310), daridorexant 25 mg (n=310), or placebo (n=310) in study 1. Between May 29, 2018, and May 14, 2020, 924 participants were randomly assigned to receive daridorexant 25 mg (n=309), daridorexant 10 mg (n=307), or placebo (n=308) in study 2. In study 1, WASO and LPS were significantly reduced among participants in the daridorexant 50 mg group compared with participants in the placebo group at month 1 (least squares mean [LSM] difference −22·8 min [95% CI −28·0 to −17·6], p<0·0001 for WASO; –11·4 min [−16·0 to −6·7], p<0·0001 for LPS) and month 3 (−18·3 min [−23·9 to −12·7], p<0·0001 for WASO; −11·7 min [−16·3 to −7·0], p<0·0001 for LPS). WASO and LPS were significantly reduced among participants in the daridorexant 25 mg group compared with the placebo group at month 1 (LSM difference −12·2 min [−17·4 to −7·0], p<0·0001 for WASO; –8·3 min [−13·0 to −3·6], p=0·0005 for LPS) and month 3 (−11·9 min [−17·5 to −6·2], p<0·0001 for WASO; −7·6 min [−12·3 to −2·9], p=0·0015 for LPS). Compared with placebo, participants in the daridorexant 50 mg group had significantly improved self-reported total sleep time at month 1 (LSM difference 22·1 min [14·4 to 29·7], p<0·0001) and month 3 (19·8 min [10·6 to 28·9], p<0·0001), and IDSIQ sleepiness domain scores at month 1 (–1·8 [–2·5 to –1·0], p<0·0001) and month 3 (–1·9 [–2·9 to –0·9], p=0·0002). Compared with the placebo group, participants in the daridorexant 25 mg group had significantly improved self-reported total sleep time at month 1 (LSM difference 12·6 min [5·0 to 20·3], p=0·0013) and month 3 (9·9 min [0·8 to 19·1], p=0·033), but not IDSIQ sleepiness domain scores (–0·8 [–1·5 to 0·01], p=0·055 at month 1; –1·0 [–2·0 to 0·01], p=0·053 at month 3). In study 2, WASO was significantly reduced among participants in the daridorexant 25 mg group compared with participants in the placebo group at month 1 (LSM difference −11·6 min [−17·6 to −5·6], p=0·0001) and month 3 (−10·3 min [−17·0 to −3·5], p=0·0028), whereas no significant differences in LPS were observed at month 1 (–6·5 min [–12·3 to –0·6], p=0·030) or month 3 (–9·0 [–15·3 to –2·7], p=0·0053). Compared with the placebo group, participants in the daridorexant 25 mg group had significant improvement in self-reported total sleep time at month 1 (LSM difference 16·1 min [8·2 to 24·0], p<0·0001) and month 3 (19·1 [10·1 to 28·0], p<0·0001), but not in IDSIQ sleepiness domain scores (–0·8 [–1·6 to 0·1], p=0·073 at month 1; –1·3 [–2·2 to –0·3], p=0·012 at month 3). Compared with the placebo group, no significant differences were observed among participants in the daridorexant 10 mg group for WASO (LSM difference –2·7 min [–8·7 to 3·2], p=0·37 at month 1; –2·0 [–8·7 to 4·8], p=0·57 at month 3), LPS (–2·6 min [–8·4 to 3·2], p=0·38 at month 1; –3·2 min [–9·5 to 3·1], p=0·32 at month 3), self-reported total sleep time (13·4 min [5·5 to 21·2], p=0·0009 at month 1; 13·6 min [4·7 to 22·5], p=0·0028 at month 3), nor IDSIQ sleepiness domain scores (–0·4 [–1·3 to 0·4], p=0·30 at month 1; –0·7 [–1·7 to 0·2], p=0·14 at month 3). Overall incidence of adverse events was comparable between treatment groups (116 [38%] of 308 participants in the daridorexant 50 mg group, 117 [38%] of 310 in the daridorexant 25 mg group, and 105 [34%] of 309 in the placebo group in study 1; 121 [39%] of 308 participants in the daridorexant 25 mg group, 117 [38%] of 306 in the daridorexant 10 mg group, and 100 [33%] of 306 in the placebo group). Nasopharyngitis and headache were the most common adverse events in all groups. One death (cardiac arrest) occurred in the daridorexant 25 mg group in study 1, which was not deemed to be treatment-related.
Interpretation
Daridorexant 25 mg and 50 mg improved sleep outcomes, and daridorexant 50 mg also improved daytime functioning, in people with insomnia disorder, with a favourable safety profile.
__________________________________________________________________________________
Multiple Early Factors Anticipate Post-Acute COVID-19 Sequelae
Yapeng Su et al
Published in Cell: Accepted: January 19, 2022 Received in revised form: December 14, 2021Received: September 29, 2021
Highlights
Post-acute sequelae of COVID-19 (PASC) represent an emerging global crisis. However, quantifiable risk-factors for PASC and their biological associations are poorly resolved. We executed a deep multi-omic, longitudinal investigation of 309 COVID-19 patients from initial diagnosis to convalescence (2-3 months later), integrated with clinical data, and patient-reported symptoms. We resolved four PASC-anticipating risk factors at the time of initial COVID-19 diagnosis: type 2 diabetes, SARS-CoV-2 RNAemia, Epstein-Barr virus viremia, and specific autoantibodies. In patients with gastrointestinal PASC, SARS-CoV-2-specific and CMV-specific CD8+ T cells exhibited unique dynamics during recovery from COVID-19. Analysis of symptom-associated immunological signatures revealed coordinated immunity polarization into four endotypes exhibiting divergent acute severity and PASC. We find that immunological associations between PASC factors diminish over time leading to distinct convalescent immune states. Detectability of most PASC factors at COVID-19 diagnosis emphasizes the importance of early disease measurements for understanding emergent chronic conditions and suggests PASC treatment strategies.
Short communication – Journal of neuroimmunology
Luke D. Liu, Deborah L. Duricka * Neuroversion Inc., Anchorage, AK, USA ARTICLE INFO
Keywords: Long COVID/PASC Myalgic encephalitis/chronic fatigue syndrome (ME/CFS) Postural orthopedic tachycardia syndrome (POTS) Dysautonomia Stellate ganglion block Cerebral blood flow
ABSTRACT After recovering from COVID-19, a significant proportion of symptomatic and asymptomatic individuals develop Long COVID. Fatigue, orthostatic intolerance, brain fog, anosmia, and ageusia/dysgeusia in Long COVID resemble “sickness behavior,” the autonomic nervous system response to pro-inflammatory cytokines (Dantzer et al., 2008). Aberrant network adaptation to sympathetic/parasympathetic imbalance is expected to produce long-standing dysautonomia. Cervical sympathetic chain activity can be blocked with local anesthetic, allowing the regional autonomic nervous system to “reboot.” In this case series, we successfully treated two Long COVID patients using stellate ganglion block, implicating dysautonomia in the pathophysiology of Long COVID and suggesting a novel treatment.
__________________________________________________________________________________
Post COVID-19 syndrome associated with orthostatic cerebral hypoperfusion syndrome, small fiber neuropathy and benefit of immunotherapy: a case report
Peter Novak 1
eNeurologicalSci . 2020 Dec;21:100276.
doi: 10.1016/j.ensci.2020.100276. Epub 2020 Sep 20.
PMID: 32984564PMCID: PMC7502253
Abstract
Coronavirus disease (COVID-19) is a novel highly contagious infectious disease caused by the coronavirus SARS-CoV2. The virus affects the human respiratory and other systems, and presents mostly as acute respiratory syndrome with fever, fatigue, dry cough, myalgia and dyspnea. The clinical manifestations vary from no symptoms to multiple organ failure. Majority of patients fully recover. Several postinfectious presumably autoimmune complications of COVID-19 affecting the brain or peripheral large nerve fibers have been reported. This report describes a post COVID-19 patient who developed chronic fatigue, orthostatic dizziness and brain fog consistent with orthostatic hypoperfusion syndrome (OCHOS), a form of orthostatic intolerance, and painful small fiber neuropathy (SFN). Initially, the patient was diagnosed with. OCHOS (detected by the tilt test with transcranial Doppler monitoring) and SFN (confirmed by skin biopsy), and both OCHOS/SFN were attributed to Post Treatment Lyme Disease Syndrome of presumed autoimmune etiology. Patient recovered on symptomatic therapy. COVID-19 triggered exacerbation of OCHOS/SFN responded to immunotherapy with intravenous immunoglobulins. This case suggests that post COVID-19 syndrome may present as an autoimmune OCHOS/SFN and that early immunotherapy may be effective. Further studies are necessary to confirm the link between OCHOS/SFN and COVID-19 disease as well as to confirm the benefit of immunotherapy.
© 2020 Published by Elsevier B.V.
__________________________________________________________________________________
PLoS One
2019 Feb 12;14(2):e0212222. doi: 10.1371/journal.pone.0212222. eCollection 2019.
Association of small fiber neuropathy and post treatment Lyme disease syndrome
Peter Novak 1, Donna Felsenstein 2, Charlotte Mao 3, Nadlyne R Octavien 4, Nevena Zubcevik 5
PMID: 30753241 PMCID: PMC6372188
Abstract
Objectives: To examine whether post-treatment Lyme disease syndrome (PTLDS) defined by fatigue, cognitive complaints and widespread pain following the treatment of Lyme disease is associated with small fiber neuropathy (SFN) manifesting as autonomic and sensory dysfunction.
Methods: This single center, retrospective study evaluated subjects with PTLDS. Skin biopsies for assessment of epidermal nerve fiber density (ENFD), sweat gland nerve fiber density (SGNFD) and functional autonomic testing (deep breathing, Valsalva maneuver and tilt test) were performed to assess SFN, severity of dysautonomia and cerebral blood flow abnormalities. Heart rate, end tidal CO2, blood pressure, and cerebral blood flow velocity (CBFv) from middle cerebral artery using transcranial Doppler were monitored.
Results: 10 participants, 5/5 women/men, age 51.3 ± 14.7 years, BMI 27.6 ± 7.3 were analyzed. All participants were positive for Lyme infection by CDC criteria. At least one skin biopsy was abnormal in all ten participants. Abnormal ENFD was found in 9 participants, abnormal SGNFD in 5 participants, and both abnormal ENFD and SGNFD were detected in 4 participants. Parasympathetic failure was found in 7 participants and mild or moderate sympathetic adrenergic failure in all participants. Abnormal total CBFv score was found in all ten participants. Low orthostatic CBFv was found in 7 participants, three additional participants had abnormally reduced supine CBFv.
Conclusions: SFN appears to be associated with PTLDS and may be responsible for certain sensory symptoms. In addition, dysautonomia related to SFN and abnormal CBFv also seem to be linked to PTLDS. Reduced orthostatic CBFv can be associated with cerebral hypoperfusion and may lead to cognitive dysfunction. Autonomic failure detected in PTLDS is mild to moderate. SFN evaluation may be useful in PTLDS.
__________________________________________________________________________________
Diverse functional autoantibodies in patients with COVID-19
Eric Y Wang # 1, Tianyang Mao # 1, Jon Klein # 1, Yile Dai # 1, John D Huck 1, Jillian R Jaycox 1, Feimei Liu 1, Ting Zhou 1, Benjamin Israelow 1, Patrick Wong 1, Andreas Coppi 2, Carolina Lucas 1, Julio Silva 1, Ji Eun Oh 1, Eric Song 1, Emily S Perotti 1, Neil S Zheng 1, Suzanne Fischer 1, Melissa Campbell 3, John B Fournier 3, Anne L Wyllie 4, Chantal B F Vogels 4, Isabel M Ott 4, Chaney C Kalinich 4, Mary E Petrone 4, Anne E Watkins 4, Yale IMPACT Team; Charles Dela Cruz 5, Shelli F Farhadian 3, Wade L Schulz 2 6, Shuangge Ma 7, Nathan D Grubaugh 4, Albert I Ko 3 4, Akiko Iwasaki 8 9 10, Aaron M Ring 11 12
PMID: 34010947 DOI: 10.1038/s41586-021-03631-y
Nature 2021 Jul;595(7866):283-288. doi: 10.1038/s41586-021-03631-y. Epub 2021 May 19
Abstract
COVID-19 manifests with a wide spectrum of clinical phenotypes that are characterized by exaggerated and misdirected host immune responses1-6. Although pathological innate immune activation is well-documented in severe disease1, the effect of autoantibodies on disease progression is less well-defined. Here we use a high-throughput autoantibody discovery technique known as rapid extracellular antigen profiling7 to screen a cohort of 194 individuals infected with SARS-CoV-2, comprising 172 patients with COVID-19 and 22 healthcare workers with mild disease or asymptomatic infection, for autoantibodies against 2,770 extracellular and secreted proteins (members of the exoproteome). We found that patients with COVID-19 exhibit marked increases in autoantibody reactivities as compared to uninfected individuals, and show a high prevalence of autoantibodies against immunomodulatory proteins (including cytokines, chemokines, complement components and cell-surface proteins). We established that these autoantibodies perturb immune function and impair virological control by inhibiting immunoreceptor signalling and by altering peripheral immune cell composition, and found that mouse surrogates of these autoantibodies increase disease severity in a mouse model of SARS-CoV-2 infection. Our analysis of autoantibodies against tissue-associated antigens revealed associations with specific clinical characteristics. Our findings suggest a pathological role for exoproteome-directed autoantibodies in COVID-19, with diverse effects on immune functionality and associations with clinical outcomes.
__________________________________________________________________________________
ORIGINAL RESEARCH article
Front. Syst. Neurosci., 01 September 2021 | https://doi.org/10.3389/fnsys.2021.698240
Acute Corticotropin-Releasing Factor Receptor Type 2 Agonism Results in Sustained Symptom Improvement in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
Gerard Pereira1*, Hunter Gillies1, Sanjay Chanda1, Michael Corbett1, Suzanne D. Vernon2, Tina Milani2 and Lucinda Bateman2
Cortene Inc., Burlingame, CA, United States 2Bateman Horne Center, Salt Lake City, UT,
Background: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a complex multi-symptom disease with widespread evidence of disrupted systems. The authors hypothesize that it is caused by the upregulation of the corticotropin-releasing factor receptor type 2 (CRFR2) in the raphé nuclei and limbic system, which impairs the ability to maintain homeostasis. The authors propose utilizing agonist-mediated receptor endocytosis to downregulate CRFR2.
Materials and Methods: This open-label trial tested the safety, tolerability and efficacy of an acute dose of CT38s (a short-lived, CRFR2-selective agonist, with no known off-target activity) in 14 ME/CFS patients. CT38s was subcutaneously-infused at one of four dose-levels (i.e., infusion rates of 0.01, 0.03, 0.06, and 0.20 μg/kg/h), for a maximum of 10.5 h. Effect was measured as the pre-/post-treatment change in the mean 28-day total daily symptom score (TDSS), which aggregated 13 individual patient-reported symptoms.
Results: ME/CFS patients were significantly more sensitive to the transient hemodynamic effects of CRFR2 stimulation than healthy subjects in a prior trial, supporting the hypothesized CRFR2 upregulation. Adverse events were generally mild, resolved without intervention, and difficult to distinguish from ME/CFS symptoms, supporting a CRFR2 role in the disease. The acute dose of CT38s was associated with an improvement in mean TDSS that was sustained (over at least 28 days post-treatment) and correlated with both total exposure and pre-treatment symptom severity. At an infusion rate of 0.03 μg/kg/h, mean TDSS improved by −7.5 ± 1.9 (or −25.7%, p = 0.009), with all monitored symptoms improving.
Conclusion: The trial supports the hypothesis that CRFR2 is upregulated in ME/CFS, and that acute CRFR2 agonism may be a viable treatment approach warranting further study.
International Journal of Environmental Research and Public Health
__________________________________________________________________________________
Impact of Life Stressors on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Symptoms: An Australian Longitudinal Study
Cassandra Balinas 1,2,3,†, Natalie Eaton-Fitch 1,2,3,†, Rebekah Maksoud 1,2,* ,† , Donald Staines 1,2 and Sonya Marshall-Gradisnik 1,2 Citation: Balinas, C.; Eaton-Fitch, N.; Maksoud, R.; Staines, D.; Marshall-Gradisnik, S. Impact of Life Stressors on Myalgic Encephalomyelitis/Chronic Fatigue Syndrome Symptoms: An Australian Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 10614. https://doi.org/10.3390/ ijerph182010614 Academic Editor: Paul B. Tchounwou Received: 1 September 2021 Accepted: 6 October 2021 Published: 11 October 2021
The National Centre for Neuroimmunology and Emerging Diseases, Menzies Health Institute Queensland, Griffith University, Gold Coast 4215, Australia;
Abstract: (1) Background: Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) is a complex, multifaceted illness. The pathomechanism, severity and progression of this illness is still being investigated. Stressors have been implicated in symptom exacerbation for ME/CFS, however, there is limited information for an Australian ME/CFS cohort. The aim of this study was to assess the potential effect of life stressors including changes in work, income, or family scenario on symptom severity in an Australian ME/CFS cohort over five months; (2) Methods: Australian residents with ME/CFS responded to questions relating to work, income, living arrangement, access to healthcare and support services as well as symptoms experienced; (3) Results: thirty-six ME/CFS patients (age: 41.25 ± 12.14) completed all questionnaires (response rate 83.7%). Muscle pain and weakness, orthostatic intolerance and intolerance to extreme temperatures were experienced and fluctuated over time. Sleep disturbances were likely to present as severe. Work and household income were associated with worsened cognitive, gastrointestinal, body pain and sleep symptoms. Increased access to healthcare services was associated with improved symptom presentation; (4) Conclusions: life stressors such as work and financial disruptions may significantly contribute to exacerbation of ME/CFS symptoms. Access to support services correlates with lower symptom scores.
__________________________________________________________________________________
The impact of COVID-19 critical illness on new disability, functional outcomes and return to work at 6 months: a prospective cohort study
Carol L. Hodgson, Alisa M. Higgins,
The COVID-Recovery Study Investigators and the ANZICS Clinical Trials Group
Critical Care volume 25, Article number: 382 (2021) Published: 08 November 2021
Abstract
Background
There are few reports of new functional impairment following critical illness from COVID-19. We aimed to describe the incidence of death or new disability, functional impairment and changes in health-related quality of life of patients after COVID-19 critical illness at 6 months.
Methods
In a nationally representative, multicenter, prospective cohort study of COVID-19 critical illness, we determined the prevalence of death or new disability at 6 months, the primary outcome. We measured mortality, new disability and return to work with changes in the World Health Organization Disability Assessment Schedule 2.0 12L (WHODAS) and health status with the EQ5D-5LTM.
Results
Of 274 eligible patients, 212 were enrolled from 30 hospitals. The median age was 61 (51–70) years, and 124 (58.5%) patients were male. At 6 months, 43/160 (26.9%) patients died and 42/108 (38.9%) responding survivors reported new disability. Compared to pre-illness, the WHODAS percentage score worsened (mean difference (MD), 10.40% [95% CI 7.06–13.77]; p < 0.001). Thirteen (11.4%) survivors had not returned to work due to poor health. There was a decrease in the EQ-5D-5LTM utility score (MD, − 0.19 [− 0.28 to − 0.10]; p < 0.001). At 6 months, 82 of 115 (71.3%) patients reported persistent symptoms. The independent predictors of death or new disability were higher severity of illness and increased frailty.
Conclusions
At six months after COVID-19 critical illness, death and new disability was substantial. Over a third of survivors had new disability, which was widespread across all areas of functioning.
Clinical trial registration NCT04401254 May 26, 2020.
__________________________________________________________________________________
Submaximal Exercise Provokes Increased Activation of the Anterior Default Mode Network During the Resting State as a Biomarker of Postexertional Malaise in Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
Rakib U. Rayhan and James N. Baraniuk
Abstract
Background: Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is characterized by disabling fatigue and postexertiona*l malaise. We developed a provocation paradigm with two submaximal bicycle exercise stress tests on consecutive days bracketed by magnetic resonance imaging, orthostatic intolerance, and symptom assessments before and after exercise in order to induce objective changes of exercise induced symptom exacerbation and cognitive dysfunction.
Method: Blood oxygenation level dependent (BOLD) scans were performed while at rest on the preexercise and postexercise days in 34 ME/CFS and 24 control subjects. Seed regions from the FSL data library with significant BOLD signals were nodes that clustered into networks using independent component analysis. Differences in signal amplitudes between groups on pre- and post-exercise days were determined by general linear model and ANOVA.
Results: The most striking exercise-induced effect in ME/CFS was the increased spontaneous activity in the medial prefrontal cortex that is the anterior node of the Default Mode Network (DMN). In contrast, this region had decreased activation for controls. Overall, controls had higher BOLD signals suggesting reduced global cerebral blood flow in ME/CFS.
Conclusion: The dynamic increase in activation of the anterior DMN node after exercise may be a biomarker of postexertional malaise and symptom exacerbation in CFS. The specificity of this postexertional finding in ME/CFS can now be assessed by comparison to post-COVID fatigue, Gulf War Illness, fibromyalgia, chronic idiopathic fatigue, and fatigue in systemic medical and psychiatric diseases.
Keywords: postexertional malaise, default mode network, DMN, blood oxygenation level dependent, BOLD, fibromyalgia, chronic idiopathic fatigue, submaximal exercise
__________________________________________________________________________________
Insights into Metabolite Diagnostic Biomarkers for Myalgic Encephalomyelitis/Chronic Fatigue Syndrome
Emi Yamano, Yasuyoshi Watanabe, and Yosky Kataoka
Abstract
Myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) is a persistent and unexplained pathological state characterized by exertional and severely debilitating fatigue, with/without infectious or neuropsychiatric symptoms, and with a minimum duration of 6 consecutive months. Its pathogenesis is not fully understood. There are no firmly established diagnostic biomarkers or treatment, due to incomplete understanding of the etiology of ME/CFS and diagnostic uncertainty. Establishing a biomarker for the objective diagnosis is urgently needed to treat a lot of patients. Recently, research on ME/CFS using metabolome analysis methods has been increasing. Here, we overview recent findings concerning the metabolic features in patients with ME/CFS and the animal models which contribute to the development of diagnostic biomarkers for ME/CFS and its treatment. In addition, we discuss future perspectives of studies on ME/CFS.
Keywords: ME/CFS, etiology, biomarker, metabolome, objective diagnosis
__________________________________________________________________________________
TRYPTOPHAN METABOLITES, CYTOKINES, AND FATTY ACID BINDING PROTEIN 2 IN MYALGIC ENCEPHALOMYELITIS/CHRONIC FATIGUE SYNDROME –
PROF. ALDO BARITUSSIO ET AL
Abstract
Patients with Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS) differ for triggers, mode of start, associated symptoms, evolution, and biochemical traits. Therefore, serious attempts are underway to partition them into subgroups useful for a personalized medicine approach to the disease.
Here, we investigated clinical and biochemical traits in 40 ME/CFS patients and 40 sex- and age-matched healthy controls.
Particularly, we analyzed serum levels of some cytokines, Fatty Acid Binding Protein 2 (FAPB-2), tryptophan, and some of its metabolites via serotonin and kynurenine.
ME/CFS patients were heterogeneous for genetic background, trigger, start mode, symptoms, and evolution. ME/CFS patients had higher levels of IL-17A (p = 0.018), FABP-2 (p = 0.002), and 3-hydroxykynurenine (p = 0.037) and lower levels of kynurenine (p = 0.012) and serotonin (p = 0.045) than controls.
Changes in kynurenine and 3-hydroxykynurenine were associated with increased kynurenic acid/kynurenine and 3-hydroxykynurenine/kynurenine ratios, indirect measures of kynurenine aminotransferases and kynurenine 3-monooxygenase enzymatic activities, respectively.
No correlation was found among cytokines, FABP-2, and tryptophan metabolites, suggesting that inflammation, anomalies of the intestinal barrier, and changes of tryptophan metabolism may be independently associated with the pathogenesis of the disease.
Interestingly, patients with the start of the disease after infection showed lower levels of kynurenine (p = 0.034) than those not starting after an infection. Changes in tryptophan metabolites and increased IL-17A levels in ME/CFS could both be compatible with anomalies in the sphere of energy metabolism.
Overall, clinical traits together with serum biomarkers related to inflammation, intestine function, and tryptophan metabolism deserve to be further considered for the development of personalized medicine strategies for ME/CFS.
__________________________________________________________________________________
BACK TO THE FUTURE? IMMUNOGLOBULIN THERAPY FOR MYALGIC ENCEPHALOMYELITIS/CHRONIC FATIGUE SYNDROME
Helen Brownlie and Nigel Speight
ABSTRACT
The findings of controlled trials on use of intravenous immunoglobulin G (IV IgG) to treat myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are generally viewed as representing mixed results. On detailed review, a clearer picture emerges, which suggests that the potential therapeutic value of this intervention has been underestimated.
Our analysis is consistent with the propositions that:
(1) IgG is highly effective for a proportion of patients with severe and well-characterised ME/CFS;
(2) responders can be predicted with a high degree of accuracy based on markers of immune dysfunction.
Rigorous steps were taken in the research trials to record adverse events, with transient symptom exacerbation commonly experienced in both intervention and placebo control groups, suggesting that this reflected the impact of participation on people with an illness characterised by post-exertional symptom exacerbation.
Worsening of certain specific symptoms, notably headache, did occur more commonly with IgG and may have been concomitant to effective treatment, being associated with clinical improvement.
The findings emerging from this review are supported by clinical observations relating to treatment of patients with severe and very severe ME/CFS, for whom intramuscular and subcutaneous administration provide alternative options.
We conclude that: (1) there is a strong case for this area of research to be revived;
(2) pending further research, clinicians would be justified in offering a course of IgG to selected ME/CFS patients at the more severe end of the spectrum. As the majority of trial participants had experienced an acute viral or viral-like onset, we further suggest that IgG treatment may be pertinent to the care of some patients who remain ill following infection with SARS-CoV-2 virus
Free full text: Healthcare
__________________________________________________________________________________
A Possible Role for Anti-idiotype Antibodies in SARS-CoV-2 Infection and Vaccination published on November 24, 2021, at NEJM.org.
William J. Murphy, Ph.D., and Dan L. Longo, M.D.
The pathogenesis of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection is incompletely understood, with its effects on multiple organ systems1 and the syndrome of “long Covid” occurring long after the resolution of infection.2 The development of multiple efficacious vaccines has been critical in the control of the pandemic, but their efficacy has been limited by the appearance of viral variants, and the vaccines can be associated with rare off-target or toxic effects, including allergic reactions, myocarditis, and immune-mediated thrombosis and thrombocytopenia in some healthy adults. Many of these phenomena are likely to be immune-mediated.3 How can we understand this diversity in immune responses in different persons?
One way of thinking about the complexity of the immune response is through the lens of anti-idiotype immune responses. The Network Hypothesis, formulated in 1974 by Niels Jerne, described a mechanism by which the antibody responses to an antigen themselves induced downstream antibody responses against the antigen-specific antibody.4 Every antibody that is induced and specific for an antigen (termed “Ab1” antibody) has immunogenic regions, particularly in their variable-region antigen-binding domains, that are unique as a result of genetic recombination of immunoglobulin variable, diversity, and joining (VDJ) genes; VDJ recombination results in new and therefore immunogenic amino acid sequences called idiotopes, which are then capable of inducing specific antibodies against Ab1 antibodies as a form of down-regulation. A similar paradigm has been proposed for T cells. However, these regulatory immune responses are also capable of doing much more. The paratopes, or antigen-binding domains, of some of the resulting anti-idiotype (or “Ab2”) antibodies that are specific for Ab1 can structurally resemble that of the original antigens themselves. Thus, the Ab2 antigen-binding region can potentially represent an exact mirror image of the initial targeted antigen in the Ab1 response, and Ab2 antibodies have even been examined for potential use as a surrogate for the antigen in vaccine studies. However, as a result of this mimicry, Ab2 antibodies also have the potential to bind the same receptor that the original antigen was targeting (Figure 1). Ab2 antibodies binding to the original receptor on normal cells therefore have the potential to mediate profound effects on the cell that could result in pathologic changes, particularly in the long term — long after the original antigen itself has disappeared.
This aspect of regulation of immune-cell responses was postulated by Plotz in 1983 as a possible cause of autoimmunity arising after viral infection5 and has since been supported experimentally by direct transfer of anti-idiotype antibodies. Ab2 antibodies generated against the enterovirus coxsackievirus B3 in mice can bind myocyte antigens, resulting in autoimmune myocarditis,6 and anti-idiotype responses can act as acetylcholine receptor agonists, leading to myasthenia gravis symptoms in rabbits.7 In addition, by displaying the mirror image of the viral antigen, Ab2 alone can even mimic the deleterious effects of the virus particle itself, as has been shown with bovine viral diarrhea virus antigen.8
For SARS-CoV-2 infection, attention centers on the spike (S) protein and its critical use of the angiotensin-converting–enzyme 2 (ACE2) receptor to gain entry into the cell. Given its critical role in regulating angiotensin responses, many physiological effects can be influenced by ACE2 engagement.9 The S protein itself has a direct effect on suppressing ACE2 signaling by a variety of mechanisms and can also directly trigger toll-like receptors and induce inflammatory cytokines.10 Anti-idiotype responses may affect ACE2 function, resulting in similar effects. However, preclinical and clinical assessments of antibody responses to SARS-CoV-2 vaccines have focused solely on Ab1 responses and virus-neutralizing efficacy. The delineation of potential anti-idiotype responses has inherent difficulties because of the polyclonal nature of responses, dynamic kinetics, and the concurrent presence of both Ab1 and Ab2 antibodies. Furthermore, ACE2 expression within cells and tissues can be variable. The different vaccine constructs (RNA, DNA, adenoviral, and protein) are also likely to have differential effects on Ab2 induction or in the mediation of vaccine effects that differ from responses to infection. Some off-target effects may not be directly linked to Ab2 responses. The association of thrombotic events with some SARS-CoV-2 vaccines in young women and the etiologic role of anti–platelet factor 4–polyanion antibodies may be the result of the adenoviral vector. However, the reported occurrence of myocarditis after vaccine administration bears striking similarities to the myocarditis associated with Ab2 antibodies induced after some viral infections.6 Ab2 antibodies could also mediate neurologic effects of SARS-CoV-2 infection or vaccines, given the expression of ACE2 on neuronal tissues, the specific neuropathologic effects of SARS-CoV-2 infection,11 and the similarity of these effects to Ab2-mediated neurologic effects observed in other viral models.
It would therefore be prudent to fully characterize all antibody and T-cell responses to the virus and the vaccines, including Ab2 responses over time. Using huACE2 transgenic mice and crossing them with strains that are predisposed to autoimmunity or other human pathologic conditions can also provide important insights. An understanding of potential Ab2 responses may also provide insights into Ab1 maintenance and efficacy and into the application of antibody-based therapeutic agents. However, much more basic science research is needed to determine the potential role idiotype-based immunoregulation of both humoral and cell-mediated responses may play both in antiviral efficacy and in unwanted side effects of both SARS-CoV-2 infection and the vaccines that protect us from it.
__________________________________________________________________________________
Graded exercise therapy for ME/CFS: finding consensus between the royal colleges, patients, and researchers
BMJ 2021; 375 doi: https://doi.org/10.1136/bmj.n3026 (Published 08 December 2021)Cite this as: BMJ 2021;375:n3026
The BMJ reports the royal colleges’ discontent with the new National Institute for Health and Care Excellence guideline on myalgic encephalomyelitis (or encephalopathy)/chronic fatigue syndrome (ME/CFS), particularly regarding graded exercise therapy (GET).12 The quality of the evidence and the rigour of its assessment are contested by the colleges, patient representatives, and researchers.34 In summary, the colleges emphasise the potential benefits of exercise for patients with ME/CFS, the patient community emphasises the potential harm that exercise can cause, and both communities quote research supporting their hypotheses, the quality of which is contested. Is there any agreement on the guideline?
Consider a patient with ME/CFS who, after attempting a therapy based on exercise, reports a worsening of their symptoms, sequelae which they regard as harmful. Should the treating physician interpret this as “the bodies [sic] normal response” and press on? Or should they defer to the NICE assertion that “treatment programmes that result in symptom exacerbation are not recommended” and abandon exercise based approaches?5
The guideline is quite clear: “Health and social care professionals should take time to build supportive, trusting, and empathetic relationships.” Trust cannot be achieved if a patient believes the prescribed treatment is causing them harm. Surely royal colleges, researchers, and patients can all agree on this?
__________________________________________________________________________________
SARS-CoV-2 spike protein S1 induces fibrin(ogen) resistant to fibrinolysis: implications for microclot formation in COVID-19
Lize M. Grobbelaar, Sample analysis, Visualization, Writing—original draft, Chantelle Venter, Data curation, Project administration, [...], and Etheresia Pretorius,
Bioscience reports Volume 41, Issue 8 – August 2021
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS-Cov-2)-induced infection, the cause of coronavirus disease 2019 (COVID-19), is characterized by unprecedented clinical pathologies. One of the most important pathologies, is hypercoagulation and microclots in the lungs of patients. Here we study the effect of isolated SARS-CoV-2 spike protein S1 subunit as potential inflammagen sui generis. Using scanning electron and fluorescence microscopy as well as mass spectrometry, we investigate the potential of this inflammagen to interact with platelets and fibrin(ogen) directly to cause blood hypercoagulation.
Using platelet-poor plasma (PPP), we show that spike protein may interfere with blood flow. Mass spectrometry also showed that when spike protein S1 is added to healthy PPP, it results in structural changes to β and γ fibrin(ogen), complement 3, and prothrombin. These proteins were substantially resistant to trypsinization, in the presence of spike protein S1. Here we suggest that, in part, the presence of spike protein in circulation may contribute to the hypercoagulation in COVID-19 positive patients and may cause substantial impairment of fibrinolysis. Such lytic impairment may result in the persistent large microclots we have noted here and previously in plasma samples of COVID-19 patients. This observation may have important clinical relevance in the treatment of hypercoagulability in COVID-19 patients.
Keywords: COVID-19, electron microscopy, Fibrin(ogen), fluorescence microscopy, Microclot, Spike protein Sa
__________________________________________________________________________________
MEDICAL NEWS: New metabolic phenotype of long COVID identified
Heather Mason | 18 January 2022
A potential new cluster phenotype for patients with post-acute COVID syndrome (PACS) is described in an article published in Open Forum Infectious Diseases, which reports on the prevalence of this metabolic-associated fatty liver disease (MAFLD) phenotype.
The analysis included 235 patients who were followed at a single university outpatient clinic. The primary outcome was the prevalence of MAFLD, detected by transient elastography, during the first post-discharge follow-up visit, compared with the MAFLD prevalence at the time of hospital admission. Figures were calculated retrospectively using the hepatic steatosis index.
The results showed that the prevalence of MAFLD was 55.3 per cent at follow-up and 37.3 per cent on admission. Among the independent predictors of MAFLD were insulin resistance (odds ratio [OR] 1.5), body mass index (OR 1.14), and metabolic syndrome (OR 2.54).
Regarding a possible link with other clusters, the researchers found that MAFLD had weak or very weak associations, indicating that it may represent an independent PACS cluster, with potential metabolic and cardiovascular health consequences in the long-COVID-19.
The authors highlight the importance of careful follow-up of patients with MAFLD in the context of PACS since it is necessary to understand the clinical implications of this syndrome.
__________________________________________________________________________________
Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis
KJETIL BJORNEVIK HTTPS://ORCID.ORG/0000-0002-2892-6986MARIANNA CORTESE HTTPS://ORCID.ORG/0000-0002-3665-2006BRIAN C. HEALY HTTPS://ORCID.ORG/0000-0001-5272-2425JENS KUHLEMICHAEL J. MINA HTTPS://ORCID.ORG/0000-0002-0674-5762YUMEI LENG HTTPS://ORCID.ORG/0000-0003-2512-9284STEPHEN J. ELLEDGE HTTPS://ORCID.ORG/0000-0001-7923-6283DAVID W. NIEBUHRANN I. SCHER[...]ALBERTO ASCHERIO
SCIENCE • 13 Jan 2022 • Vol 375, Issue 6578 • pp. 296-301 • DOI: 10.1126/science.abj8222
Stronger evidence for viral connection
Multiple sclerosis is a chronic demyelinating disease of the central nervous system. The underlying cause of this disease is not known, but Epstein-Barr virus is thought to be a possible culprit. However, most people infected with this common virus do not develop multiple sclerosis, and it is not feasible to directly demonstrate causation of this disease in humans. Using data from millions of US military recruits monitored over a 20-year period, Bjornevik et al. determined that Epstein-Barr virus infection greatly increased the risk of subsequent multiple sclerosis and that it preceded the development of disease, supporting its potential role in the pathogenesis of multiple sclerosis (see the Perspective by Robinson and Steinman). —YN
Abstract
Multiple sclerosis (MS) is a chronic inflammatory demyelinating disease of the central nervous system of unknown etiology. We tested the hypothesis that MS is caused by Epstein-Barr virus (EBV) in a cohort comprising more than 10 million young adults on active duty in the US military, 955 of whom were diagnosed with MS during their period of service. Risk of MS increased 32-fold after infection with EBV but was not increased after infection with other viruses, including the similarly transmitted cytomegalovirus. Serum levels of neurofilament light chain, a biomarker of neuroaxonal degeneration, increased only after EBV seroconversion. These findings cannot be explained by any known risk factor for MS and suggest EBV as the leading cause of MS.
__________________________________________________________________________________
FDA OKs New Adult Insomnia Med - Medscape medical news
Erik Greb
January 10, 2022
The US Food and Drug Administration (FDA) has approved the dual orexin receptor antagonist daridorexant (Quviviq) for the treatment of insomnia in adults, the drug's manufacturer, Idorsia, has announced.
The FDA's decision was based partly on a phase 3 trial of adults with moderate-to-severe insomnia who were randomly assigned to receive 25 or 50 mg of daridorexant or matching placebo. Daridorexant was associated with dose-dependent improvements in wake after sleep onset, total sleep time, and latency to persistent sleep.
Whereas the overall results are very positive, the improvements in daytime functioning are especially "exciting," Thomas Roth, PhD, director of the Sleep Disorders and Research Center at Henry Ford Hospital in Detroit, Michigan, told Medscape Medical News.
"That's sort of a big deal. For me, that's the biggest deal there is," said Roth, who was a consultant on the design of the phase 3 trial and on the interpretation of the data.
The drug will be available in doses of 25 mg and 50 mg, and the FDA has recommended that it be classified as a controlled substance. After it is scheduled by the US Drug Enforcement Administration, daridorexant is expected to be made available in May.
Favorable Safety Profile
Insomnia is a common disorder characterized by difficulty falling asleep or staying asleep and by early morning awakenings. Patients with insomnia often report fatigue, irritability, and difficulty with concentration. The condition can also result in significant problems with work and social activities, thus contributing to anxiety or depression.
As with other dual orexin receptor antagonists, daridorexant competitively binds with both orexin receptors in the lateral hypothalamus to block the activity of orexin in a reversible way. This approach decreases the downstream action of the wake-promoting neurotransmitters that are overactive in patients with insomnia.
The phase 3 trial measured daytime functioning using the new Insomnia Daytime Symptoms and Impacts Questionnaire (IDSIQ), a patient-reported outcome instrument. Daridorexant was associated with significant improvements in daytime function, particularly in sleepiness and mood.
Previous trials of other dual orexin receptor antagonists did not use the IDSIQ as an outcome, so it is not possible to compare daridorexant with those drugs in this respect, Roth noted. Researchers also have not conducted head-to-head trials of the drug with other dual orexin receptor antagonists.
Daridorexant also had a favorable safety profile and was not associated with rebound insomnia or withdrawal effects. The most common adverse events were headache and somnolence or fatigue.
"They had no effect on sleep stage distribution [and] they had no significant effects on sleep and breathing in people with mild to moderate sleep apnea," said Roth, who presented the phase 3 findings at SLEEP 2020.
__________________________________________________________________________________
The Lancet: ARTICLES| VOLUME 21, ISSUE 2, P125-139, FEBRUARY 01, 2022
Safety and efficacy of daridorexant in patients with insomnia disorder: results from two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials
- Prof Emmanuel Mignot, MD David Mayleben, PhD Prof Ingo Fietze, MD Damien Leger, MD Gary Zammit, PhD Claudio L A Bassetti, MD et al.
Summary
Background
Daytime functioning is impaired in people with insomnia disorder. Currently available dual orexin receptor antagonists have shown efficacy in insomnia disorder, but do not address all aspects of this disease. We aimed to assess safety and efficacy of daridorexant, a novel orexin receptor antagonist, on night-time and daytime symptoms of insomnia.
Methods
We did two multicentre, randomised, double-blind, placebo-controlled, phase 3 trials at 156 sites in 17 countries. Adults (aged ≥18 years) with insomnia disorder were randomly assigned using interactive response technology (1:1:1) to receive daridorexant 50 mg, 25 mg, or placebo (study 1) or daridorexant 25 mg, 10 mg, or placebo (study 2) every evening for 3 months. Participants, investigators, and site personnel were masked to treatment allocation. The primary endpoints were change from baseline in wake time after sleep onset (WASO) and latency to persistent sleep (LPS), measured by polysomnography, at months 1 and 3. The secondary endpoints were change from baseline in self-reported total sleep time and the sleepiness domain score of the Insomnia Daytime Symptoms and Impacts Questionnaire (IDSIQ) at months 1 and 3. Study-wise type I error rate (5%) was controlled for all pairwise comparisons. Efficacy was analysed in all randomly assigned participants, and safety in all participants who received at least one dose of treatment. The studies are registered at ClinicalTrials.gov, NCT03545191 (study 1) and NCT03575104 (study 2).
Findings
Between June 4, 2018 and Feb 25, 2020, 930 participants were randomly assigned to receive daridorexant 50 mg (n=310), daridorexant 25 mg (n=310), or placebo (n=310) in study 1. Between May 29, 2018, and May 14, 2020, 924 participants were randomly assigned to receive daridorexant 25 mg (n=309), daridorexant 10 mg (n=307), or placebo (n=308) in study 2. In study 1, WASO and LPS were significantly reduced among participants in the daridorexant 50 mg group compared with participants in the placebo group at month 1 (least squares mean [LSM] difference −22·8 min [95% CI −28·0 to −17·6], p<0·0001 for WASO; –11·4 min [−16·0 to −6·7], p<0·0001 for LPS) and month 3 (−18·3 min [−23·9 to −12·7], p<0·0001 for WASO; −11·7 min [−16·3 to −7·0], p<0·0001 for LPS). WASO and LPS were significantly reduced among participants in the daridorexant 25 mg group compared with the placebo group at month 1 (LSM difference −12·2 min [−17·4 to −7·0], p<0·0001 for WASO; –8·3 min [−13·0 to −3·6], p=0·0005 for LPS) and month 3 (−11·9 min [−17·5 to −6·2], p<0·0001 for WASO; −7·6 min [−12·3 to −2·9], p=0·0015 for LPS). Compared with placebo, participants in the daridorexant 50 mg group had significantly improved self-reported total sleep time at month 1 (LSM difference 22·1 min [14·4 to 29·7], p<0·0001) and month 3 (19·8 min [10·6 to 28·9], p<0·0001), and IDSIQ sleepiness domain scores at month 1 (–1·8 [–2·5 to –1·0], p<0·0001) and month 3 (–1·9 [–2·9 to –0·9], p=0·0002). Compared with the placebo group, participants in the daridorexant 25 mg group had significantly improved self-reported total sleep time at month 1 (LSM difference 12·6 min [5·0 to 20·3], p=0·0013) and month 3 (9·9 min [0·8 to 19·1], p=0·033), but not IDSIQ sleepiness domain scores (–0·8 [–1·5 to 0·01], p=0·055 at month 1; –1·0 [–2·0 to 0·01], p=0·053 at month 3). In study 2, WASO was significantly reduced among participants in the daridorexant 25 mg group compared with participants in the placebo group at month 1 (LSM difference −11·6 min [−17·6 to −5·6], p=0·0001) and month 3 (−10·3 min [−17·0 to −3·5], p=0·0028), whereas no significant differences in LPS were observed at month 1 (–6·5 min [–12·3 to –0·6], p=0·030) or month 3 (–9·0 [–15·3 to –2·7], p=0·0053). Compared with the placebo group, participants in the daridorexant 25 mg group had significant improvement in self-reported total sleep time at month 1 (LSM difference 16·1 min [8·2 to 24·0], p<0·0001) and month 3 (19·1 [10·1 to 28·0], p<0·0001), but not in IDSIQ sleepiness domain scores (–0·8 [–1·6 to 0·1], p=0·073 at month 1; –1·3 [–2·2 to –0·3], p=0·012 at month 3). Compared with the placebo group, no significant differences were observed among participants in the daridorexant 10 mg group for WASO (LSM difference –2·7 min [–8·7 to 3·2], p=0·37 at month 1; –2·0 [–8·7 to 4·8], p=0·57 at month 3), LPS (–2·6 min [–8·4 to 3·2], p=0·38 at month 1; –3·2 min [–9·5 to 3·1], p=0·32 at month 3), self-reported total sleep time (13·4 min [5·5 to 21·2], p=0·0009 at month 1; 13·6 min [4·7 to 22·5], p=0·0028 at month 3), nor IDSIQ sleepiness domain scores (–0·4 [–1·3 to 0·4], p=0·30 at month 1; –0·7 [–1·7 to 0·2], p=0·14 at month 3). Overall incidence of adverse events was comparable between treatment groups (116 [38%] of 308 participants in the daridorexant 50 mg group, 117 [38%] of 310 in the daridorexant 25 mg group, and 105 [34%] of 309 in the placebo group in study 1; 121 [39%] of 308 participants in the daridorexant 25 mg group, 117 [38%] of 306 in the daridorexant 10 mg group, and 100 [33%] of 306 in the placebo group). Nasopharyngitis and headache were the most common adverse events in all groups. One death (cardiac arrest) occurred in the daridorexant 25 mg group in study 1, which was not deemed to be treatment-related.
Interpretation
Daridorexant 25 mg and 50 mg improved sleep outcomes, and daridorexant 50 mg also improved daytime functioning, in people with insomnia disorder, with a favourable safety profile.
__________________________________________________________________________________
Multiple Early Factors Anticipate Post-Acute COVID-19 Sequelae
Yapeng Su et al
Published in Cell: Accepted: January 19, 2022 Received in revised form: December 14, 2021Received: September 29, 2021
Highlights
- Longitudinal multiomics associate PASC with autoantibodies, viremia and comorbidities
- Reactivation of latent viruses during initial infection may contribute to PASC
- Subclinical autoantibodies negatively correlate with anti-SARS-CoV-2 antibodies
- Gastrointestinal PASC uniquely present with post-acute expansion of cytotoxic T cells
Post-acute sequelae of COVID-19 (PASC) represent an emerging global crisis. However, quantifiable risk-factors for PASC and their biological associations are poorly resolved. We executed a deep multi-omic, longitudinal investigation of 309 COVID-19 patients from initial diagnosis to convalescence (2-3 months later), integrated with clinical data, and patient-reported symptoms. We resolved four PASC-anticipating risk factors at the time of initial COVID-19 diagnosis: type 2 diabetes, SARS-CoV-2 RNAemia, Epstein-Barr virus viremia, and specific autoantibodies. In patients with gastrointestinal PASC, SARS-CoV-2-specific and CMV-specific CD8+ T cells exhibited unique dynamics during recovery from COVID-19. Analysis of symptom-associated immunological signatures revealed coordinated immunity polarization into four endotypes exhibiting divergent acute severity and PASC. We find that immunological associations between PASC factors diminish over time leading to distinct convalescent immune states. Detectability of most PASC factors at COVID-19 diagnosis emphasizes the importance of early disease measurements for understanding emergent chronic conditions and suggests PASC treatment strategies.
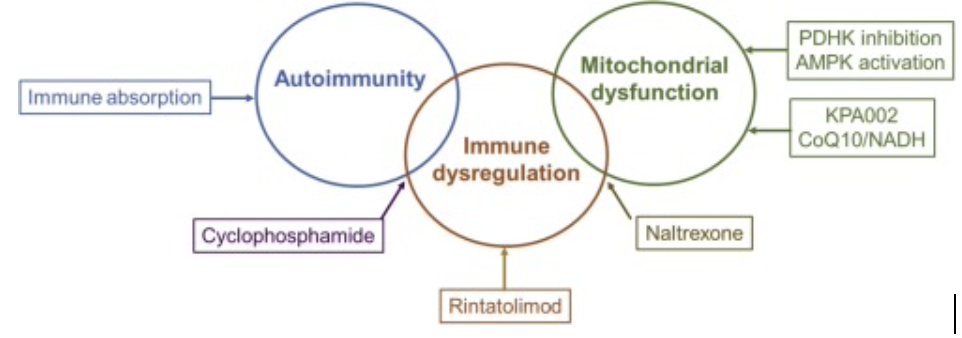
 RSS Feed
RSS Feed